A distal radius fracture—often called a “broken wrist”—is one of the most common upper limb fractures we see in the clinic, especially after a fall onto an outstretched hand (FOOSH). But what most people don’t realise is that not all wrist fractures are the same—and neither is their treatment. Some need surgery, others don’t. Some heal quickly, others become lifelong problems if poorly managed.
In this guide, we’ll unpack:
- The different types of distal radius fractures
- What most people don’t know about them
- The complications that can occur without proper rehab
- Why early input from a hand therapist can be the difference between a great recovery and persistent dysfunction
🧠 Not All Wrist Fractures Are the Same: Types & Nuances
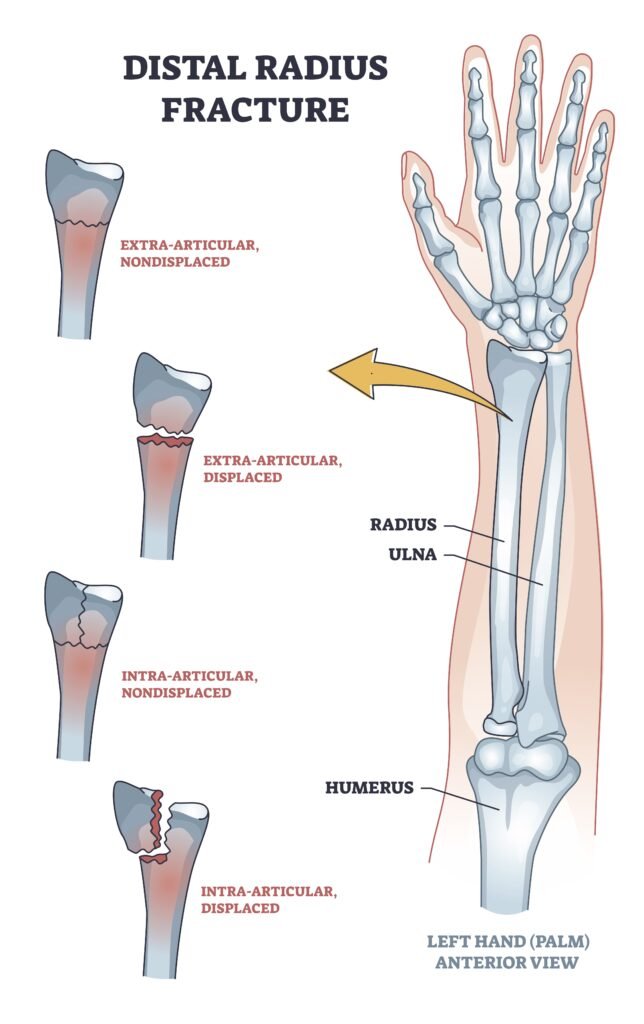
The distal radius is the end of your forearm bone near the wrist. When it fractures, the pattern of the break can vary greatly depending on:
- Age and bone quality
- Direction and force of the impact
- Whether the break is intra-articular (involving the joint surface) or extra-articular
Common Fracture Patterns:
- Colles fracture: The classic break where the fragment is displaced dorsally (towards the back of the hand). Common in older adults after a FOOSH.
- Smith’s fracture: The opposite of a Colles—fragment shifts volarly (toward the palm). Often from a fall onto a flexed wrist.
- Barton’s fracture: An intra-articular fracture with dislocation—often unstable and requires surgery.
- Chauffeur’s fracture (Radial styloid fracture): A fracture of the radial styloid, sometimes missed on initial X-rays.
What Most Don’t Realise:
- Even “minor” fractures can disrupt joint mechanics. If the articular surface is not perfectly aligned (within ~2mm step-off), it increases the risk of post-traumatic arthritis.
- Loss of radial height or tilt can lead to long-term weakness, limited supination/pronation, and altered load-bearing through the wrist.
😮 Things Most People Don’t Know About Distal Radius Fractures
- 🧩 Fracture displacement doesn’t always correlate with pain severity. Some patients have significant displacement but minimal symptoms early on.
- 🔄 Malunion can affect the elbow and shoulder. When the wrist doesn’t heal properly, patients often unconsciously adjust how they move their arm, potentially leading to secondary issues up the kinetic chain.
- 🧠 DRUJ instability (Distal Radioulnar Joint) is often overlooked—particularly in fractures that extend into the ulnar notch. This can impair forearm rotation long after the fracture “heals.”
- 🕵️♂️ Associated soft tissue injuries are common but under-diagnosed, especially injuries to the TFCC (Triangular Fibrocartilage Complex), scapholunate ligament, or ulnar styloid.
- 🖐️ Nerve irritation (like median nerve neuropathy) can mimic or mask symptoms of a fracture, especially if swelling or displacement compresses the carpal tunnel.
🧭 Why Thoughtful Rehab Matters for a Great Outcome
While bones generally heal well, a well-guided recovery can make all the difference in how confidently you return to work, sport, or daily life. Addressing the finer details—like joint alignment, tendon mobility, and strength—can help avoid common hurdles in the recovery journey.
A few things we aim to support during your rehab:
| Focus Area | Why It Matters | How We Help |
|---|---|---|
| Wrist alignment & mobility | Restores natural wrist mechanics and load distribution | Hands-on therapy, joint mobilisation, custom splinting if needed |
| Forearm rotation & DRUJ function | Essential for tasks like opening jars or turning keys | Specific exercises to restore rotation and stabilise the joint |
| Tendon and nerve health | Promotes smooth movement and prevents irritation | Guided tendon gliding, sensory re-education, swelling control |
| Grip strength and endurance | Crucial for work, sport, and confidence using your hand | Progressive loading, functional retraining |
| Comfort and confidence | Reduces stiffness and empowers you to trust your wrist again | Education, reassurance, tailored exercises that match your pace |
Many people are surprised by how quickly they adapt and regain strength once rehab is tailored to their needs. By working with a hand therapist, you’ll have someone who understands the intricacies of wrist recovery and can guide you each step of the way.
💡 Why Seeing a Hand Therapist Early Matters
Many people assume that once the cast is off, they’re “good to go.” But recovery doesn’t end there. In fact, that’s when the real work begins.
A hand therapist:
- Guides early mobilisation while protecting the healing structures
- Assesses for DRUJ instability, tendon gliding, and scar adhesions
- Provides tailored strengthening, proprioception, and return-to-function training
- Can fabricate a custom splint to address stiffness or instability
- Monitors for signs of complications like CRPS or tendon rupture
Compared to general physiotherapy, hand therapists have specialised training in the anatomy, biomechanics, and rehab of the hand and wrist—critical when millimetres matter.
💪 The Road to Recovery: What to Expect
| Phase | What Happens | What You Need |
|---|---|---|
| 0–6 weeks | Immobilisation (cast or splint) | Elevation, edema control, finger movement |
| 6–12 weeks | Fracture consolidation | Guided wrist mobilisation, scar work |
| 12–24 weeks | Strength and function return | Grip training, return to sport/work planning |
| 6+ months | Full recovery or chronic issues appear | Ongoing rehab for any residual deficits |

📍Your Wrist Deserves Better Than “Wait and See”
If you’ve broken your wrist—or are struggling with pain or dysfunction after a distal radius fracture—it’s not just about healing the bone. It’s about restoring full function, preventing complications, and getting your life back.
👉 Book your appointment with our expert hand therapy team today.
Let’s get your wrist moving again—safely, efficiently, and with confidence.